CLINICAL EFFECTIVENESS OF NON-INVASIVE SELECTIVE CRYOLIPOLYSIS
JIEHOON KIM 1, DAI HYUN KIM 2 & HWA JUNG RYU 2
1Dr. Kim ’ s Skin & Laser Clinic, Dermatology, Suwon, Republic of Korea and 2Department of Dermatology, Korea University College of Medicine, Seoul, Republic of Korea
Journal of Cosmetic and Laser Therapy, 2014; 16: 209–213
Contents
Abstract
Background: Excess subcutaneous fat causes not only cosmetic issues, but also substantial systemic health problems. Cryolipolysis has been reported to provide non-invasive fat reduction that significantly reduces subcutaneous fat cells with controlled, localized cooling.
Objective: This study is intended to determine whether a cryolipolysis device can effectively reduce subcutaneous fat without damaging the overlying skin or causing significant side effects and ultimately produce improved cosmetic results.
Materials and methods: A total of 15 patients participated in this study and they were treated unilaterally in a split-body trial manner with a non-invasive cryolipolysis device (Micool™, Hironic Co., Seongnam, Korea). The degree of improvement was assessed by both objective and subjective assessments. Complications and side effects were recorded at every visit.
Results: The results of both objective and subjective assessments showed significant improvements in subcutaneous fat reduction without any meaningful complications.
Conclusion: Non-invasive selective cryolipolysis has been reported to be a safe and effective treatment modality for the reduction of excess adipose tissue. Therefore, cryolipolysis is a promising technology that could be an appropriate and safe therapeutic option for subcutaneous fat reduction.
INTRODUCTION
Unwanted excess subcutaneous fat negatively impacts not only body shape and image, but also causes various chronic diseases. Therefore, concerns of the public, physicians, and scientists have been growing, and the media has been promoting the image of a slim body as the virtue of beauty and health.
Among the numerous therapeutic modalities that have been developed so far, liposuction still remains the most common surgical cosmetic procedure. Although liposuction is an effective therapeutic option for the removal of fat and can be safely performed as an outpatient procedure, it is an invasive method with surgical risks, such as infection, scarring, hematoma, deep vein thrombosis, and pulmonary embolism, in addition to the specific risks associated with general anesthesia (1,2).
A non-invasive procedure that also enables effective fat removal is necessary because of the potential side effects of liposuction. Many such non-invasive treatment methods have been developed, including endermologie (LPG Systems, Valence, France), radiofrequency treatment, and light-based treatment (lasers or low level light therapy)(3 – 5). However, the therapeutic results of these methods are not as satisfactory and they are therefore used as adjunct methods to liposuction. High intensity focused ultrasound (HIFU) is regarded as a treatment that safely and effectively reduces subcutaneous fat tissues (6); however, it is still difficult to use widely because of the pain and high cost of consumable devices.
Non-invasive selective cryolipolysis is a new technology that uses cold exposure or energy extraction to cause localized panniculitis and fat modulation. This technology is based on clinical observations that cold exposure, under the proper circumstances, can result in localized panniculitis. This panniculitis ultimately results in the reduction and clearance of adipose tissue without injury to the surrounding normal tissue (7). Micool™ (Hironic Co., Seongnam, Korea) is a non-invasive selective cryolipolysis device and was approved by the Ministry of Food and Drug Safety (MFDS) of the Korean government in 2013. Several articles have been published reporting the efficacy of non-invasive devices (Zeltiq Aesthetics, Pleasanton, CA), but nothing has been documented related to Micool™, despite its growing clinical usage in Korea. This study aimed to determine the effectiveness of the Micool™ cryolipolysis device and ensure that it does not damage the overlying skin or cause significant side effects.
MATERIALS AND METHODS
The subjects in this study were patients who visited Dr. Kim ’ s Skin & Laser Clinic from April to November, 2013. Eligible subjects were men and women who were older than 20 years of age with more than a moderate degree of obesity. Potential subjects were excluded if they had received liposuction or another surgical procedure in the intended treatment area; had a history of subcutaneous injections into the area within the past 4 weeks; had a history of chronic disease such as hypertension, diabetes, or hyperlipidemia; had a significant psychiatric problem such as body dysmorphism; or had taken diet pills within the past 4 weeks. Individuals who were pregnant or lactating were also excluded from the study.
Potential side effects were fully explained to the patients prior to treatment and these included erythema, bruising, and neurologic complications such as tenderness, dulling of sensation or numbness, and tingling. These expected complications and other possibly related findings were documented directly after treatment as well as 3 months after each procedure. They all agreed to the use of their photos and informed consent was obtained from all of the patients.
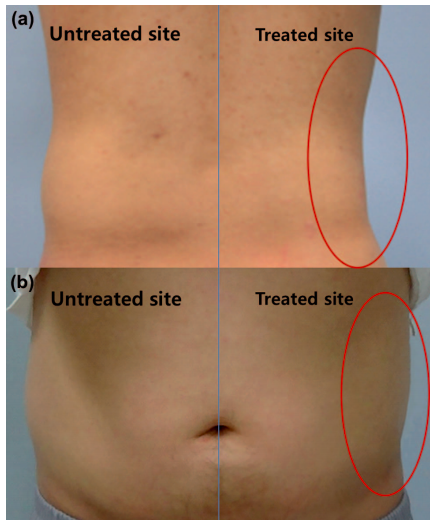
The targeted treatment sites were visible fat on the flanks (‘love handles’), lower abdomen (belly), upper chest (bra-line), upper hip, under the buttocks, or inner thigh (Figure 1B). In principle, the cryolipolysis device was eventually applied to both sides of the targeted area; however, sequential split-body trials were done for more accurate comparison of clinical efficacy. In detail, individuals received treatment on one side and the following procedure was completed after 3 months of close observation. Each patient met with the medical assistant for baseline photographs, after which the physician performed cryolipolysis. Digital photographic images were documented under controlled conditions with the same light source, room, and camera before the treatment and during each session. The patients were treated with a non-invasive selective cryolipolysis device using a cooling intensity factor (CIF) of 33 (-64 mW/cm 2) for 60 minutes per application site. CIF is the index representing the rate of heat flux into or out of the tissue opposite the cooling device.
In this study, all subjects were requested to revisit the clinic for clinical photographs and assessment 2 weeks, 1 month, 2 months, and 3 months after each procedure. The results of the cryolipolysis treatment were analyzed using both subjective evaluations by the patients and objective assessments by the physicians. Objective improvement was assessed with clinical photography after the final session and 3 months thereafter on a 5-point scale as follows: 1=excellent improvement or >75% subcutaneous fat reduction, 2=good improvement or 50 – 75% subcutaneous fat reduction, 3=fair improvement or 25 – 50% subcutaneous fat reduction, 4=noticeable improvement or 10 – 25% subcutaneous fat reduction, 5=no improvement or 0 – 10% subcutaneous fat reduction. The data collected at baseline and 3 months post-treatment were compared for a final estimation of the clinical value. The objective assessment was performed by two independent and experienced dermatologists. The subjective assessment was obtained with a questionnaire composed of a 5-point scale as follows: 1=significantly satisfactory, 2=moderately satisfactory, 3=slightly satisfactory, 4=moderately unsatisfactory, and 5=significantly unsatisfactory.
Statistical analysis was performed using SPSS version 19.0 for Windows (Statistical Package for the Social Sciences, SPSS, Chicago, USA). The paired t-test was used for evaluation of statistical significance between the scores of both objective and subjective assessments at baseline and 3 months after treatment. Differences were considered statistically significant when p <0.05.
RESULTS
Initially, 18 patients volunteered to participate in the study; however, 3 patients were conclusively excluded from the study due to loss to follow-up. The reason for loss to follow-up was not related to results of the procedure, such as unsatisfactory outcomes or complications, and was due to personal affairs. A total of 15 patients (11 women and 4 men) fulfilled all of the requirements of the investigation. The mean age was 30.1 years, with a range of 22 to 41. Treatments were delivered primarily to the love handles (40.0%, n=6), belly (20.0%, n=3), upper hip (13.3%,n=2), inner thigh (13.3%, n=2), bra line (6.7%, n=1), and under the buttocks (6.7%, n=1). Patient information and assessment outcomes are described in Table I.
The treatments delivered to different anatomic sites were also analyzed by gender. Men almost exclusively received treatment to the love handles (50.0%, n=2) and belly (50.0%, n=2). Women, in comparison, received treatment over a much wider range of areas, including the love handles (36.4%, n=4), upper hip (18.2%, n=2), inner thigh (18.2%, n=2), bra line (9.1%, n=1), belly (9.1%, n=1), and under the buttocks (9.1%, n=1). The treatment sites were also analyzed by patient age range. The patients were divided into 2 groups, 20 to 29 years old and more than 30 years old. The number of patients in each group was similar, with 8 for the former and 7 for the latter; however, the composition was quite different. The treatment sites of the former group were love handles (37.5%, n=3), upper hip (25.0%, n=2), inner thigh (25.0%, n=2), and banana muffin (12.5%, n=1). The latter group received treatments of the love handles (42.9%, n=3), belly (42.9%, n=3), and bra line (14.3%, n=1). It can be assumed that both groups were interested in treatment of the love handles, but the younger group desired modification of the thigh or hip area and the older group was more concerned with their belly.
Results of both the objective and subjective assessments were revealed to be statistically significant (p < 0.05) compared to the baseline state. The average point of the objective assessment was 1.7, which implies good to excellent improvement or 50% to 100% subcutaneous fat reduction. The average of the subjective assessment was 2.1, indicating moderately satisfactory results. The assessments were also analyzed by gender and treatment site. The average values of the objective and subjective assessments of male patients were 1.5 and 1.8, respectively. The average points for female subjects were 1.8 and 2.2, respectively. It seemed that the male patients showed slightly more favorable results with cryolipolysis than their female counterparts. The most satisfactory treatment site was area under the buttocks, followed by the love handle. The average values for the objective and subjective assessments of under the buttocks were 1.0 and 1.0, and the love handle showed points of 1.3 and 1.5, respectively. Clinical photos of love handle treatment by cryolipolysis are described in Figure 1. The male patients received cryolipolysis treatment once on the right and once on the left love handle area. After 3 months, they all showed excellent improvement and expressed significant satisfaction with the results. The most dissatisfactory area was the bra line followed by the inner thigh. The average values for both the objective and subjective assessments of the bra line were 3.0 and 4.0, respectively, and the values for the inner thigh were 2.0 and 3.0, respectively. Each subject was closely observed and managed for possible complications during the entire course of the study. All patients experienced immediate erythema (Figure 2a) and minor pain for several hours, but these symptoms vanished within one day without specific management. Bruising (Figure 2b) emerged in some patients at the treatment site and disappeared within 2 to 5 days without further treatment. Neurologic complications, such as tenderness, dulling of sensation or numbness, or tingling sensation, were not reported until 3 months after the last procedure. All patients were also shown to have no other long-lasting symptoms or discomfort at the last questionnaire 3 months after the last treatment.
CONCLUSION
In conclusion, non-invasive selective cryolipolysis appears to be a safe and effective treatment option for the reduction of excess adipose tissue. Although the exact pathophysiology of cryolipolysis should be verified by further research, cryolipolysis is still a promising technology that could be an appropriate and safe therapeutic option to resolve a serious health and psychosocial problem: obesity.
REFERENCES
- Alderman AK, Collins ED, Streu R, Grotting JC, Silkin AL, Neligan P, et al. Benchmark outcomes in plastic surgery: National complication rates for abdominoplasty and breast augmentation. Plast Reconstr Surg. 2009 ; 124 : 2127 – 2133.
- Desrosiers AE III, Grant RT, Breitbart AS. Don’t try this at home: Liposuction in the kitchen by an unqualified practitioner leads to disastrous complications. Plast Reconstr Surg. 2004 ; 113 : 460 – 461 .
- Güleç AT. Treatment of cellulite with LPG endermologie. Int J Dermatol. 2009 ; 48 : 265 – 270
- Anderson RR, FarinelliW, Laubach H, Manstein D, Yaroslavsky AN, GubeliJ III, et al. Selective photothermolysis of lipid-rich tissues: a free electron laser study. Lasers Surg Med. 2006 ; 38 : 913 – 919 .
- Narins RS, Tope WD, Pope K, Ross EV. Overtreatment effects associated with a radiofrequency tissue-tightening device: rare, preventable, and correctable with subcision and autologous fat transfer. Dermatol Surg. 2006 ; 32 : 115 – 124 .
- Teitelbaum SA, Burns JL, Kubota J, Matsuda H, Otto MJ, Shirakabe Y, et al. Noninvasive body contouring by focused ultrasound: Safety and efficacy of the Contour Idevice in a multicenter, controlled, clinical study. Plast Reconstr Surg. 2007 ; 120 : 779 – 789 .
- Manstein D, Laubach H, Watanabe K, FarinelliW, ZurakowskiD, Anderson RR. Selective cryolysis: a novel method of non-invasive fat removal. Lasers Surg Med. 2008 ; 40 : 595 – 604 .
- Rotman H. Cold panniculitis in children: adiponecrosis E frigore of Haxthausen. Arch Dermatol. 1996 ; 94 : 720 – 721 .
- Zelickson B, Egbert BM, Preciado J, Allison J, Springer K, Rhoades RW, Manstein D. Cryolipolysis for noninvasive fat cell destruction: initial results from a pig model. Dermatol Surg. 2009 ; 35 : 1462 – 1470.
- Shek SY, Chan NP, Chan HH. Non-invasive cryolipolysis for body contouring in Chinese-a first commercial experience. Lasers Surg Med. 2012 ; 44 : 125 – 130.
- Stevens WG, Pietrzak LK, Spring MA. Broad overview of a clinical and commercial experience with CoolSculpting. Aesthet Surg J. 2013 ; 33 : 835 – 846.
Avram MM, Harry RS. Cryolipolysis for subcutaneous fat layer reduction. Lasers Surg Med. 2009 ; 41 : 703 – 708. - Nelson AA, Wasserman D, Avram MM. Cryolipolysis for reduction of excess adipose tissue. Semin Cutan Med Surg. 2009 ; 28 : 244–249.
- Klein KB, Zelickson B, Riopelle JG, Okamoto E, Bachelor EP, Harry RS, Preciado JA. Non-invasive cryolipolysis for subcutaneous fat reduction does not affect serum lipid levels or liver function tests. Lasers Surg Med. 2009 ; 41 : 785 – 790.
- Coleman SR, Sachdeva K, Egbert BM, Preciado J, Allison J. Clinical efficacy of non-invasive cryolipolysis and its effects on peripheral nerves. Aesthetic Plast Surg. 2009 ; 33 : 482 – 488.